
Eyelid
Blepharospasm
Diagnosis and treatment of essential blepharospasm and hemifacial spasm — including botulinum toxin injection and surgical myectomy.
Medically reviewed by Morris E. Hartstein, MD, FACSOculoplastic SurgeonLast updated June 2026
Eyelid
Diagnosis and treatment of essential blepharospasm and hemifacial spasm — including botulinum toxin injection and surgical myectomy.
Medically reviewed by Morris E. Hartstein, MD, FACSOculoplastic SurgeonLast updated June 2026
Blepharospasm refers to involuntary, forceful closure of the eyelids due to sustained or intermittent contraction of the orbicularis oculi muscle. It ranges from mild, occasional blinking to severely debilitating functional blindness from inability to open the eyes. Two distinct conditions are treated by oculoplastic surgeons: essential blepharospasm and hemifacial spasm.
Blepharospasm and hemifacial spasm are neurological conditions — initial evaluation often involves both neurology and oculoplastic surgery. Related conditions include Lagophthalmos (a separate problem of incomplete closure) and Eyelid Laxity.
Essential blepharospasm (EB) is a focal dystonia — an involuntary movement disorder — characterized by bilateral, synchronous, sustained contraction of the orbicularis oculi. It begins subtly with increased blinking or mild lid spasm and can progress to near-complete functional blindness.
▶ What Blepharospasm Looks Like
Patient education: a patient with benign essential blepharospasm — involuntary, forceful spasms of the eyelids. (This video shows the condition itself, not a treatment.)
Essential blepharospasm results from abnormal activity in the basal ganglia-thalamo-cortical circuitry, leading to excessive activation of the orbicularis oculi. It is not a primary eye condition but a central motor control disorder. Dry eye and ocular surface irritation can trigger or worsen spasm, which is why addressing ocular surface disease is part of comprehensive management.
Hemifacial spasm (HFS) is a distinct condition caused by aberrant pulsatile compression of the facial nerve (CN VII) at its root exit zone from the brainstem, typically by a blood vessel (most commonly the anterior inferior cerebellar artery (AICA) or posterior inferior cerebellar artery (PICA)). This results in unilateral, involuntary contractions of the facial muscles.
MRI with gadolinium is recommended to evaluate the cerebellopontine angle and identify neurovascular compression. MRI also excludes mass lesions or demyelinating disease at the root exit zone.
Clinical history and examination are central to diagnosis. The pattern (bilateral vs. unilateral), age of onset, progression, and associated neurological symptoms guide workup.
Botulinum toxin injection is the first-line treatment for both essential blepharospasm and hemifacial spasm. It is highly effective and generally well tolerated, with most patients obtaining meaningful symptom relief.
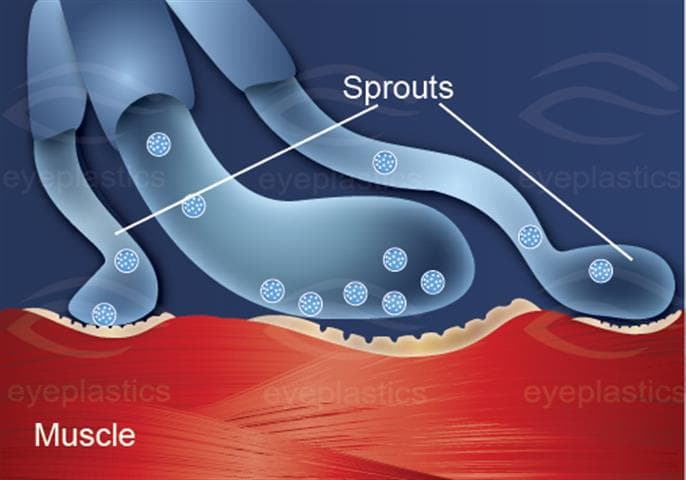
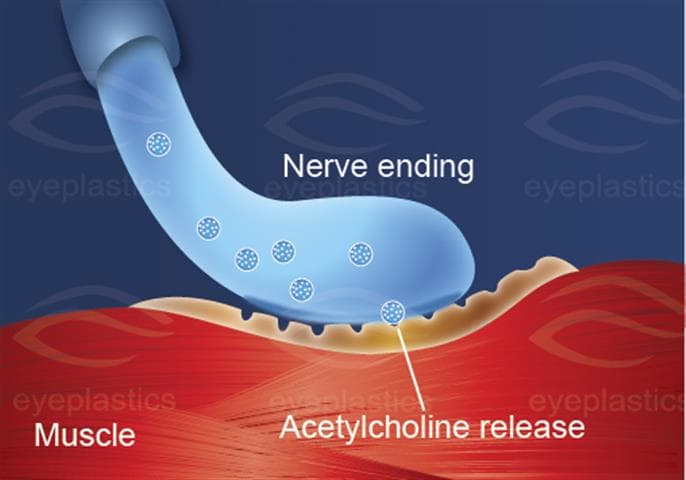
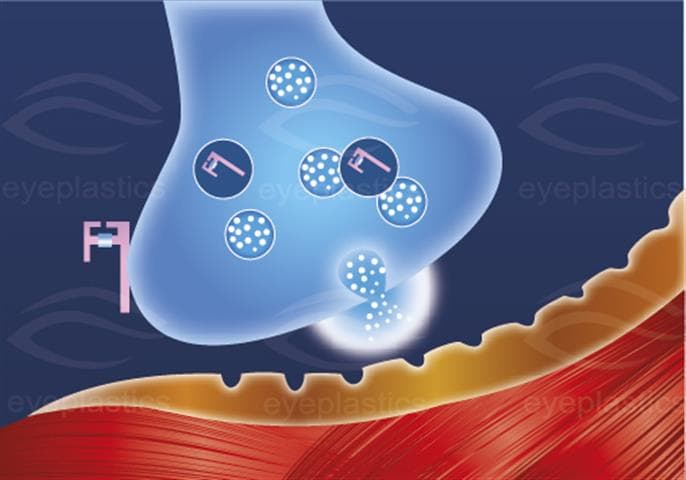
Botulinum toxin type A (onabotulinumtoxinA — Botox; abobotulinumtoxinA — Dysport; incobotulinumtoxinA — Xeomin) blocks acetylcholine release at the neuromuscular junction, producing a temporary, reversible chemical denervation of the injected muscle. For blepharospasm, small amounts are injected into the pretarsal and preseptal orbicularis oculi bilaterally.
Mechanism of Action — Illustrated
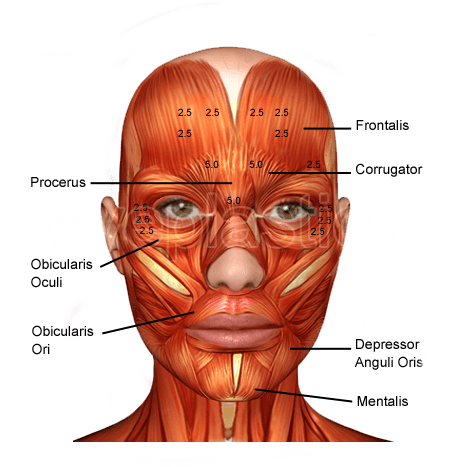
For patients with essential blepharospasm who have inadequate response to botulinum toxin, or who cannot tolerate injections, surgical myectomy is an option. The procedure involves excision of the orbicularis oculi, corrugator supercilii, and procerus muscles through upper and lower eyelid incisions.
For hemifacial spasm refractory to botulinum toxin, microvascular decompression (MVD) — a neurosurgical procedure — is curative in 85–95% of cases when neurovascular compression is confirmed on MRI. This is performed by a neurosurgeon.
Blepharospasm is a chronic condition, and connecting with others who live with it makes a real difference. These organizations offer education, support communities, and research updates:
Schedule a consultation with Morris E. Hartstein, MD, FACS to learn if this procedure is right for you.